
Introduction of Treatment Cases for Lymphedema Patients (Same-day LVA Surgery and Conservative Therapy)
Case Studies
We provide a lifetime of support through a combined treatment of LVA surgery, optimal conservative therapy, and rehabilitation. To make an appointment with Dr. Mihara, please click here.
Same-day surgery is performed at Lymphedema Clinic, Tokyo. Inpatient surgery and rehabilitation will be done at JR Tokyo General Hospital.

We have also created a medical manga (cartoon) to help patients and their families understand our practice. Please take a moment to read it!
Our medical team determines a treatment plan tailored to each patient’s goals. Here are some typical cases. We have also created a medical manga (cartoon) to help patients and their families understand our practice. Please take a moment to read it!
Information for lymphedema patients suffering from cellulitis is available here.
For information on early lymphedema (prophylactic LVA), click here.
Lower Extremity Lymphedema


A female in her 60s with bilateral lower extremity lymphedema after uterine cancer surgery
The patient underwent radical hysterectomy, lymph node dissection, and radiation therapy for cervical cancer 18 years ago. Lymphedema appeared in both lower limbs post-operatively, and the symptoms gradually worsened despite conservative treatment. In the past few years, cellulitis (fever of about 40°C) occurred around 4 times a year. With persistent lymphorrhea from the back of the lower leg and the inner thigh, she had great difficulty performing compression therapy and having a social life. After receiving 2 lymphatic venous anastomosis procedures from our medical team under local anesthesia, she can now perform compression therapy, with cellulitis no longer occurring. Not only did edema improve, but lymphorrhea also disappeared.
Key Point 1: Appropriate Diagnostic Imaging

Our practice team determines a therapeutic strategy based on the patient’s medical data to meet the goals of each patient.
For this reason, we believe it’s important for patients to know about their lymphatic function. Our clinic performs lymphoscintigraphy on all patients to evaluate their lymphatic functions before deciding on a treatment plan. The above patient was suffering from significant edema. However, good lymphatic function remained, and LVA (Lymphatic Venous Anastomosis) surgery was performed after the effectiveness of the surgery was confirmed.
Key Point 2: Extensive Medical Data
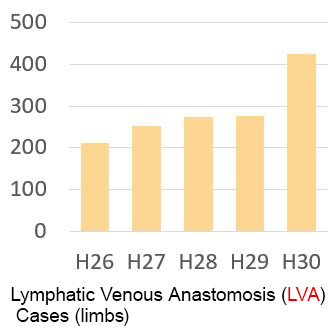
Our medical team has performed over 400 Lymphatic Venous Anastomosis (LVA) procedures (limbs) per year/as of 2008. In all cases, we conduct scientific analysis of therapeutic efficacy and strive daily to improve treatment outcomes. Based on this abundant treatment data, we determine a therapeutic strategy for each patient. Conventionally, lymphedema treatment was focused on behavioral restrictions such as “sleeping with your legs elevated,” “giving up on hot springs,” and “avoiding sports.”
Our therapeutic strategy is to provide appropriate treatment (conservative therapy, weight loss, surgical treatment) so patients can enjoy their daily lives proactively. Some of our patients work full-time standing, while some run marathons, climb mountains, or challenge taking a round-the-world trip. One 80-year-old patient enjoys her daily life of Japanese dance and ballroom dancing. The accumulation of a wealth of scientific data has significantly changed the treatment of lymphedema.
Key Point 3: Multidisciplinary Teamwork

Our clinic values the cooperative activities of the physicians specializing in lymphedema and a team of lymphedema therapists. Our analysis of 10 years of treatment data shows that only about 7% of patients respond significantly to surgical treatment alone. Appropriate conservative therapy and body weight control are key to maximizing the effectiveness of treatment.
For this reason, cooperating with professionals with various skills, knowledge, and experience is essential.
Lower Extremity Lymphedema
This patient, a female in her 50s with lymphedema (after uterine cancer surgery), visited us from Aomori prefecture (northern Japan). She came to us because there was no local medical facility where she could be treated for lymphedema. In addition to having cellulitis about 3 times a year, she refrained from going out to a minimum, being afraid of developing cellulitis. She stayed at home for longer hours, which caused stress, leading to gaining weight over time. As she gained weight, her lymphedema continued to exacerbate.


Lymphatic Venous Anastomosis (LVA) was confirmed effective by evaluating the lymphatic function before surgery using lymphoscintigraphy. After LVA was performed under local anesthesia and the cellulitis development was controlled, the patient was hospitalized at JR Tokyo General Hospital for about 4 weeks to strengthen conservative therapy and weight control. After confirming that her heart could withstand the exercise load, the exercise intensity gradually increased. She was eventually discharged from the hospital when she could enjoy sports with the general public at the Jexer Gym at Shinjuku, affiliated with JR Tokyo General Hospital.
Since discharge, she has not developed cellulitis, continues to lose weight, and her edema continues to improve. After returning to Aomori, she is enjoying sports in her daily life. Her edema and cellulitis improved with a combination of surgical treatment, conservative therapy, and physiotherapy.
Treatment for Primary Lower Extremity Lymphedema

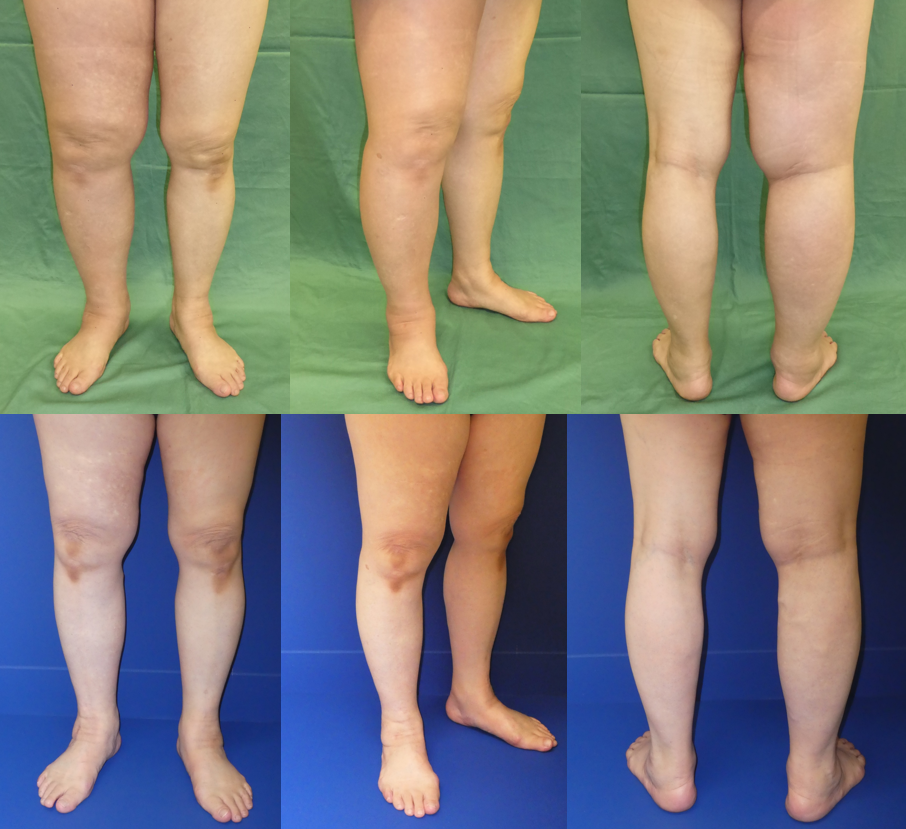
A female in her 20s. She was referred to our team after the appearance of edema of unknown cause in both lower extremities, especially around the Achilles tendon, which other medical institutions could not diagnose.
Lymphoscintigraphy showed lymph node atrophy of unknown cause, and she was diagnosed with primary lymphedema.
The patient was treated with a combination of LVA and conservative therapy.
Before the treatment (upper row), the patient was psychologically depressed, which led her to quit her job and be confined at home. After the treatment (lower row), she regained a positive state psychologically. She has resumed her job, does workouts at a fitness club every week, and has a healthy life. She is also enjoying fashion.
Even for lymphedema of unknown cause, our team will make an appropriate diagnosis and treatment plan using diagnostic imaging (including lymphoscintigraphy, ICG lymphangiography, and lymphatic ultrasound). Based on these test results, we support our patients by providing various approaches such as surgery, appropriate stocking instructions by a lymph therapist, and rehabilitation by a physical therapist, depending on the patient’s wishes and goals in rebuilding their lives.
Treatment Point 1 (Controlling Cellulitis)

Our medical team has compiled scientific data to indicate that treating lymphatic venous anastomosis (LVA) reduces the probability of cellulitis (redness and pain in the affected area and systemic fever of 38.5°C or higher) to approximately 1/8 (one-eighth). Currently, our successful treatment outcomes exceed 90%. We recommend LVA for patients who develop cellulitis more than twice a year. Once the cellulitis is under control, conservative treatment can be strengthened for more stable treatment of edema, cellulitis, and pain.
Treatment Point 2 (Proposal of Less Stressful Treatment for the Body)


Our practice team performs Lymphatic Venous Anastomosis (LVA) under local anesthesia. The surgical incision is only about 1 to 3 cm, making this procedure very easy on the patient. It can be safely operated even on patients over 90 years of age or those with heart problems.
By using preoperative ultrasound (echo) and ICG fluorescence lymphography, we can accurately examine the location, size, and function of the collecting lymphatic vessels and the veins to be anastomosed. The outcome of anastomosis in 10 sites 10 years ago and the current results of anastomosis in 3 sites are comparable. By performing these diagnostic imaging procedures before surgery, the operation time has been reduced by half (approximately 2.5 to 3 hours), and the size and number of wounds have also decreased. We can identify good lymphatic vessels even in patients with severe lymphedema.
Treatment Point 3 (Combination of Exercise Therapy and Weight Control)
Lower Extremity Lymphedema Radical Operation for Elephantiasis (Liposuction)

A female in her 30s who underwent uterine cancer surgery. We at Lymphedema Clinic Tokyo perform radical operations for elephantiasis (under general anesthesia) for post-LVA patients with enlarged residual adipose tissue, working with the Department of Lymphatic/Reconstructive Surgery of JR Tokyo General Hospital to remove the enlarged fat tissue. Based on prior ultrasonography, fat is removed mainly in areas where the lymphatic vessels have disappeared. There is no fat removal in areas where lymphatic vessels remain. We can remove abnormally enlarged adipose tissue by adopting ultrasonography while preserving the lymphatic vessel function.
Treatment Point 4 (Ultrasound-guided Radical Operation for Elephantiasis)

Using ultrasound, the condition of the lymphatic vessels can be determined in detail. The fat-removal area is mainly on areas where the collecting lymphatic vessels are absent.
Treatment Point 5 (Combined with LVA)

Our medical team performs radical operations for elephantiasis after lymphatic venous anastomosis (LVA) by improving the lymphatic flow and then removing enlarged adipose tissue, resulting in a more stable postoperative outcome.
Case A (Right upper limb lymphedema after right mastectomy)

Patient Summary
The patient had undergone right total mastectomy and axillary lymph node dissection followed by radiation therapy 12 years previously due to breast cancer. Right upper limb lymphedema appeared after the surgery and continued to exacerbate regardless of any conservative treatment. Cellulitis with an associated fever of 40℃ or higher occurred once a month in the most recent few years and the symptoms had impaired the patient from doing any daily activities. We performed lymphatic venous anastomosis surgery under local anesthesia followed by the continuation of post-operative conservative therapy. The patient’s lymphedema gradually improved and cellulitis is no longer observed.
Study Cases
Surgical plans are made for each patient based on lymphatic function (lymphoscintigraphy results). By appropriately combining conservative therapy and surgery (such as LVA), we can treat extremely severe lymphedema cases, which were considered difficult to treat in the past. Please refer to the description below.







[I want to live well to be 100 years old!]
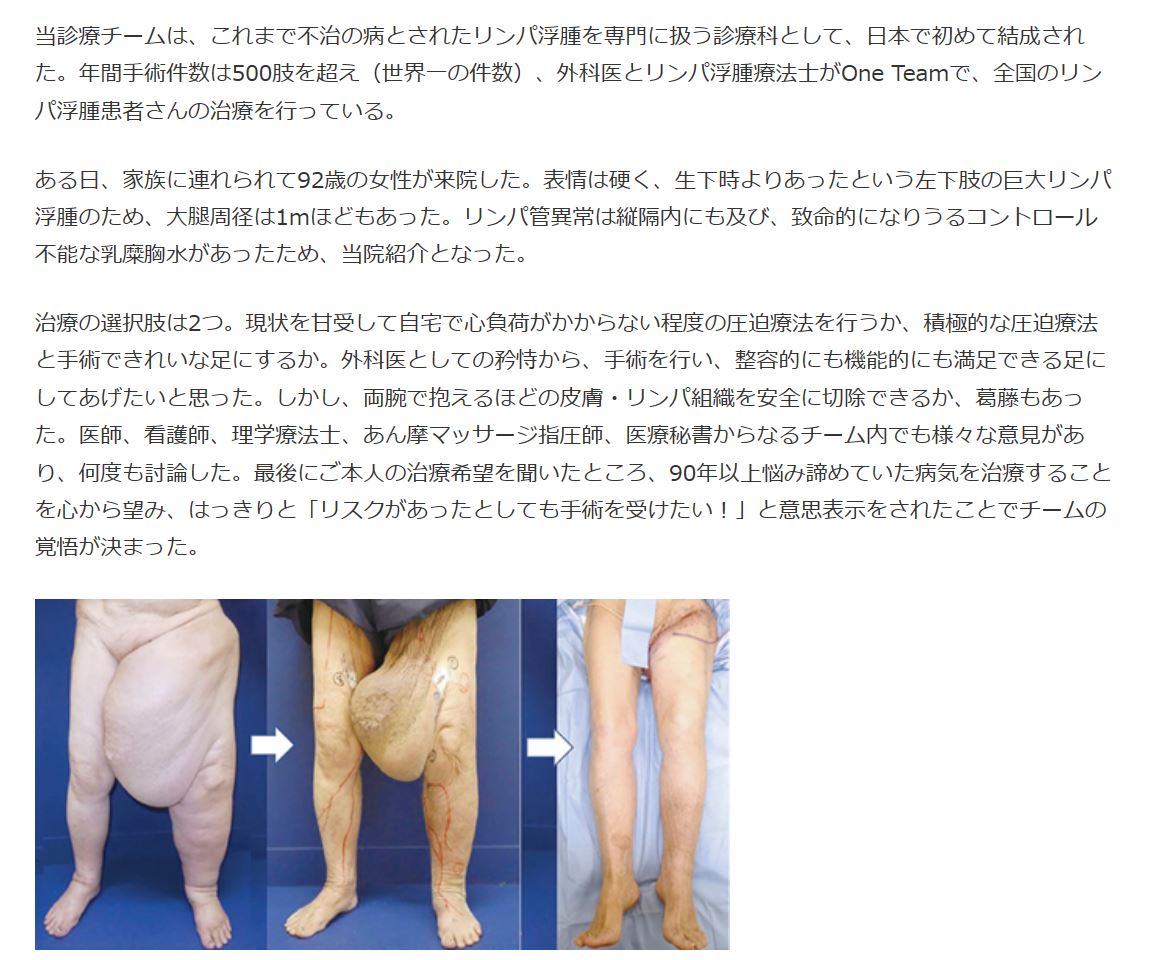
Lymphatic Surgical Treatment for an older female (92-year-old)
We combine minimally invasive lymphatic surgical treatment with conservative therapy customized to each patient’s lymphatic function. This is an introduction to a case in which we treated extremely severe lymphedema in an older female over 90 years of age. The patient (see below) was born with a very severe lymphedema and chylothorax. She had suffered from these diseases all her life. She was treated at many hospitals but could not be cured and was over 90 years old when her doctor referred her to our clinic as a last resort. We treated her, and with her, the treatments consisted of Lymphatic Venous Anastomosis (LVA / operation time of 2 hours) under local anesthesia and removal of excess skin under lumbar anesthesia and local anesthesia as the second surgery.
The treatment went smoothly, and the patient’s lymphedema improved to almost normal. She chose soccer for the rehabilitation exercise she had wanted to do before and was discharged from the hospital in good health. Since the patient was in her 90s and had chylothorax, conservative therapy was started with low pressure while checking her general condition.
Before the treatment, she used a wheelchair to move around in the hospital, but after the treatment, she could walk powerfully on her own feet, saying, “I will live well to 100 years old! !”
Our medical team is dedicated to providing safe treatment without making unreasonable surgical plans. In this case, we believe a good treatment outcome was achieved due to the cooperative efforts of doctors, nurses, physical therapists, occupational therapists, licensed masseurs, and medical secretaries. Photos and videos are publicized with the patient’s permission.
“We gotta do somethin about lymphedema!” This is the message we want to deliver to elderly patients.

An article on our practice was featured in Weekly Medical News on May 18, 2020 (for more details, click here ).



Collaborating with Clinics Specializing in Conservative Therapy
We collaborate with a clinic specializing in lymphedema (ana Clinic/Kawagoe City). The patient shown below underwent LVA after conservative treatment at ana Clinic. The patient’s edema condition has improved, and she is glad she regained the will to live. We recommend that once a patient is diagnosed with lymphedema, the patient visits a specialized medical institution or treatment facility to strengthen conservative treatment. For more details about ana Clinic, click here. Our practice team is very confident in this center.
[In-home medical care collaboration]
Bethel South Shinjuku Clinic offers nearby residents conservative treatment and in-home medical care.
If you wish to receive medical care at home, we will provide treatment by coordinating with Town Home Care Clinic (*Click here to check the areas where visits are available).

LVA Surgery for Early Lymphedema and Lymphedema Prevention

Our medical team recommends early treatment for patients with early-stage lymphedema and very early-stage lymphedema after lymph node dissection for the following three reasons.
First, an early LVA surgery can prevent the condition from deteriorating (accumulation of scientific evidence).
Second, it is now possible to identify abnormal dilation of lymphatic vessels by lymphoscintigraphy, ICG testing, and ultrasonography before edema develops. Once the lymphatic abnormality is identified, LVA surgery is performed to prevent the development of lymphedema.
Third, we believe that prevention of lymphedema for young patients (in their 20s to 40s) who have had uterine cancer treatment is critical, considering their lives for the next 40 to 60 years. By receiving LVA, patients can enjoy athletic activities at peace and prevent cancer recurrence (click here for more information).
The above figure shows LVA surgery performed on a female in her 40s by our team.
Lymphoscintigraphy shows that the preoperative dermal backflow areas (abnormal findings) have improved after the operation. Patients with a good postoperative course can minimize the conservative
care including wearing compression stockings. Depending on the patient’s condition, stockings or sleeves may no longer be necessary.
Treatment for Genital Lymphedema and Genital Lymphatic Vesicles
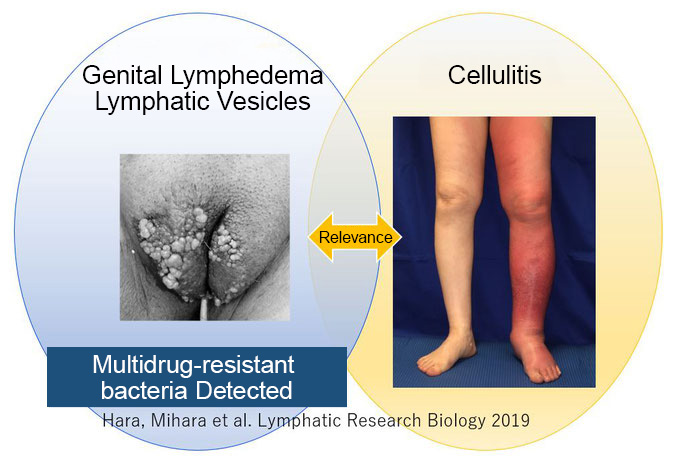
Our practice team provides treatment for “genital lymphedema and genital lymphatic vesicles” by a female physician.
Genital lymphedema and genital lymphatic vesicles are difficult to diagnose and are often misdiagnosed as condyloma acuminatum (sexually transmitted disease).
Genital lymphatic vesicles, particularly, are a factor in the development of cellulitis and require proper diagnosis and treatment.
We provide an explanation of the therapeutic strategy after making a definitive diagnosis using lymphoscintigraphy.
As for genital lymphatic vesicles, treatment will be given at JR Tokyo General Hospital. For more therapeutic information, click here (Dr. Naoko Hara’s website).
Lymphedema Clinic Tokyo treats patients with excessively severe lymphedema in cooperation with JR Tokyo General Hospital.
We propose treatment tailored to each patient’s condition, combining conservative therapy and surgical treatment (such as LVA).
We have treated many patients with extremely severe lymphedema who had difficulty not just walking but even standing, enabling them to stand and walk.
We provide medical care with the hope of seeing a smile on the faces of patients who have given up on treatment. *The photos and videos are publicized with the patient's consent.